
Time to go into the light...
Ehrlichiosis &
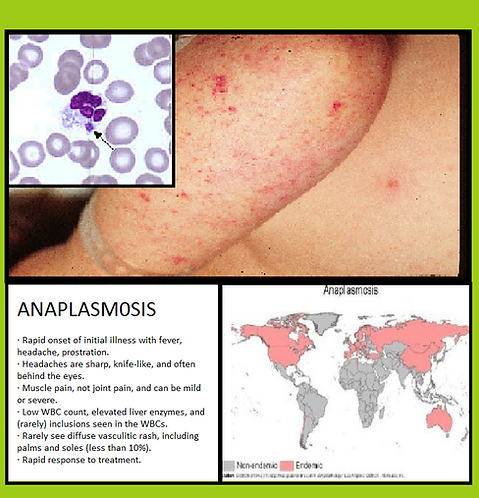
Anaplasmosis

Ehrlichiosis is caused by various types of Ehrlichia and Anaplasmosis is caused by Anaplasma phagocytophilum.
Ehrlichiosis was formerly called HME, human monocytic ehrlichiosis and Anaplasmosis used to be called HGE, human granulocytic ehrlichiosis.
Some studies suggest that, in endemic areas, as many as 15 – 36% of the human population has been infected, although many people may not be aware that they are infected.
The clinical manifestations of ehrlichiosis and anaplasmosis are the same. Each is often characterized by sudden high fever, fatigue, muscle aches, headache. Rash is uncommon but has been reported. The disease can be mild or life-threatening. Severely ill patients can have low white blood cell count, low platelet count, anemia, elevated liver enzymes, kidney failure and respiratory insufficiency. Older people or people with immune suppression are more likely to require hospitalization. Deaths have occurred.
Compared with HME, HGA appears less likely to involve the central nervous system, but peripheral neuropathies are more common and can last weeks to months. Among the neurologic findings reported in the medical literature are facial palsy, demyelinating polyneuropathy and brachial plexopathy. Respiratory distress syndrome and a septic or toxic shock-like syndrome have been reported, but appear to be less common than in HME.Diagnosis is limited by our current ability to test for only two species. Ehrlichia parasites multiply inside host cells, forming large mulberry-shaped clusters called morulae that doctors can sometimes see on blood smears. The infection still can easily be missed. The doctor may suspect ehrlichiosis or anaplasmosis in a patient who does not respond well to treatment for Lyme disease.
Treatment like Lyme Disease is dependent on where you live and who is your doctor. Here are several treatment protocols;
Center for Disease Control (CDC)
Doxycycline is the first line treatment for adults and children of all ages and should be initiated immediately whenever anaplasmosis is suspected.
Use of antibiotics other than doxycycline or other tetracyclines has been associated with a higher risk of fatal outcome for some rickettsial infections. Doxycycline is most effective at preventing severe complications from developing if it is started early in the course of disease. Therefore, treatment must be based on clinical suspicion alone and should always begin before laboratory results return.
If the patient is treated within the first 5 days of the disease, fever generally subsides within 24-72 hours. In fact, failure to respond to doxycycline suggests that the patient’s condition might not be due to anaplasmosis. Severely ill patients may require longer periods before their fever resolves. Resistance to doxcycline or relapses in symptoms after the completion of the recommended course have not been documented.
Recommended Dosage
Doxycycline is the first line treatment for adults and children of all ages:
-
Adults: 100 mg every 12 hours
-
Children under 45 kg (100 lbs): 2.2 mg/kg body weight given twice a day
Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement. Standard duration of treatment is 7 to 14 days. Some patients may continue to experience headache, weakness and malaise for weeks after adequate treatment.
ASSOCIATION OF MEDICAL MICROBIOLOGY AND
INFECTIOUS DISEASE (AMMI) CANADA
AMMI Canada’s review concludes that the IDSA guideline is in alignment with the published
evidence on Lyme disease and with other Lyme disease management guidelines and is free of
inherent bias.
National Collaborating Center for Infectious Diseases (Canada)
Human Granulocytic Anaplasmosis – HGA is transmitted by I. scapularis and I. pacificus in North America, and its distribution tracks that of Lyme disease at a much lower incidence [58]. It causes flu-like symptoms that are typically more severe than in early Lyme disease, plus thrombocytopenia, leukopenia, and increased liver enzymes; HGA has no distinctive symptom and requires laboratory confirmation for diagnosis [59]. This zoonosis is becoming established in southwestern Quebec [60]. Between 2.3% and 10% of patients presenting with erythema migrans (acute Lyme disease) are co-infected with HGA [61]. Treatment for HGA is the same as for Lyme disease.
Canadian Lyme Disease Foundation
Diagnosing ehrlichiosis is difficult because currently available tests can identify only two species of the parasite. Ehrlichiaparasites multiply inside host cells, forming large mulberry-shaped clusters called “morulae”, which can sometimes be seen in a blood sample, but the infection still can be missed. Diagnosis of Anaplasmosis is usually by PCR of the bacterium in the blood.
Doctors sometimes identify and diagnose ehrlichiosis / anaplasmosis when patients don’t respond well to treatment for Lyme disease.
The treatment of choice for ehrlichiosis / anaplasmosis is doxycycline, with rifampin recommended in case of treatment failure.
Columbia University Medical Centre
The optimal dose and duration of antibiotic treatment for anaplasmosis has not been definitively established, but it is clear that A. phagocytophilum is highly sensitive to tetracyclines. Thus, oral doxycycline is the recommended treatment, at the same dose used for Ehrlichia infections: 200 mg/day in two divided doses. The usual treatment duration is 5-10 days, which is extended if there is suspected coinfection with B. burgdorferi, the agent of Lyme disease. In any case, treatment should continue for at least three days after the patient’s fever resolves. Response to treatment is usually rapid; if the patient remains febrile more than two or three days after initiation of doxycycline therapy, the diagnosis should be revisited.
As with Ehrlichia infections, Rifampin is used in cases where doxycycline is contraindicated, such as pregnancy or allergy. Rifampin has also been used successfully in pediatric cases, and thus is sometimes employed in mild cases of pediatric A. phagocytophilum infection. If coinfection with B. burgdorferi is suspected in a pediatric case, doxycycline is sometimes used as an initial treatment for 3-5 days, with another antibiotic employed thereafter to complete the somewhat longer recommended treatment period for early Lyme disease.
other sources sited
https://www.lymedisease.org/lyme-basics/co-infections/ehrlichia-and-anaplasma/