
Time to go into the light...
CDC "Fear Mongering"
Long term antibiotics safe for all but Lyme disease
In response to a series of fear mongering articles floating around the media, whether it be from the Chicago Tribune with their warning about “Lyme literate health professionals taking advantage of anyone falling the illusion of “Lyme Loonies” and thinking they have chronic Lyme and not a number of other serious health conditions.
or directly from the masters of media manipulation and purveyors of pharm filtered facts; the CDC ( Center for Disease Control) or as I prefer to call them Corrupt Doctors’ Corp. It discloses the CDC’s concern that individuals are being put at risk with physicians diagnosing them with “chronic Lyme disease” is used by some health care providers as a diagnosis for various constitutional, musculoskeletal, and neuropsychiatric symptoms.
“Dangerous unproven treatments for 'chronic Lyme disease' are on the rise”

"An increasing number of Americans with medically ambiguous symptoms are being misdiagnosed with "chronic Lyme disease" and prescribed dangerous treatments."
“Serious Bacterial Infections Acquired During Treatment of Patients Given a Diagnosis of Chronic Lyme Disease"

The article outlines the same 5 incidences of treatment failure, one ending in death; as its logic for being against long term antibiotic treatment in any residual symptoms of Lyme. When I went to look at each of these cases I noticed that all involved the use of IV or antibiotic delivery. And it wasn’t the medication but the delivery method that created negative outcomes. So what is the truth about long term antibiotic use? What really happens when they are taken for an extended period of time outside the CDC and PHAC Lyme treatment guidelines? What do we really need to be considering when we talk about more than 28 days of Doxycycline?
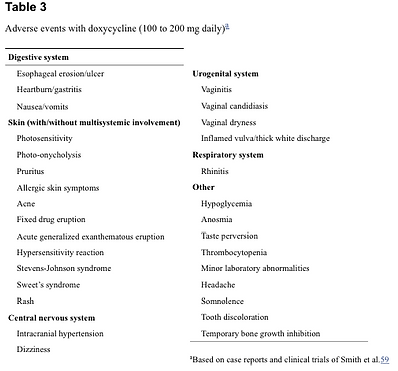
I will start with the most obvious concern to consider when taking any pharmaceutical; what are the side effects?
Making informed consent and taking anything needs to start with all the facts, not just those that support any one dogma. Perhaps my ability to play devil’s advocate has made me ability to take more than one view and consider the information in between opposing perspectives. If I only have one source of information on any topic my concept is very limited. The more time I take looking into multiple angles the more accurate my assessment can be.
I am not a personal fan of most antibiotics because of the negative impact they naturally have on the microbiome.
If we look at antibiotics like bombs sent into to arm the immune system and annihilate the enemy. Some antibiotics are more specific than other in the type of target intruder cell they are aimed at, but none are what we would consider a 'Smart Bomb' reducing only harmful pathogens and leveling the rest of the site of infection intact and undisturbed. Recent studies and document have acknowledged collectively that the “Being” known as human is actually more “non-human” or bacterial than human DNA cells.
That what have been considered “germs” because of their bacterial or viral cell structures. Scientists are just starting to map the variety of microbes that go into various different bodily functions, but they know that these “germs”/pathogens are needed for our very existence.
I used to feel that there were the good the bad and the ugly when it came to various pathogens, suggesting that some needed to be eliminated or eradicated, after spending some time digging deeper, I have changed my mind. Wonderful thing about being a woman is that is perfectly allowed. I now look at bacteria and viruses as functional or dysfunctional, suggesting that all can be addressed by balancing the microbiome. The question is what is the best way to do so?

If we review the effect of the pathogen killing nature of antibiotics, we need to consider the collateral damage to helpful or beneficial bacterial or viral microbes. Each antibiotic is known to cause an imbalance of needed probiotics needed to maintain health. For every action there is a reaction, thusly is the intrinsic nature of most antibiotics.
There are significant sized lists of possible physical outcomes or side effects one might have to endure while taking antibiotics; these are most likely issue resulting from the imbalances and faulty signaling happening to the microbiome in the gut.
A knowledgeable physician will understand the need for supporting the microbiome if it is antibiotics that are needed. I believe that having a healthy microbiome allows the immune system to function at optimum which reduces the need to take more aggressive treatment and use antibiotics. Having health is the presence of optimal functioning in all areas, not the absence of disease. Most “DIS” ease is multifaceted and isn’t as simplistic as eliminating one offending microbe. Health should be a pursuit involving diet, lifestyle, stress reduction and management, nutrient intake and absorption, family history and whatever individual aspects that make the patient an individual. The allotted 8-15 mins afforded most doctors does not permit the sharing of information needed to look at the WHOLE person , leaving most to address the symptom and not the cause of the imbalance in that patients life.
I think that antibiotics should be a line of defense when the person is losing the battle with their own immune system, mostly I believe that if antibiotics are absolutely needed, that they are given with clear dietary instructions on how to support the microbiome during use.


Devil's Advocate
Successful Long-term Antibiotics Use
So as a good Advocate, I need to consider the opposite side, so let’s look at the science that says about Doxycycline and long term use. I was actually surprised that there are several reports suggesting that long term/extended (more than 28 days) use of Doxy has no more negative impact than that of taking 28 days or less.
Treatment for OAL (Ocular adnexal lymphoma)
A study examining “Ocular adnexal lymphoma (OAL) has been associated with Chlamydophila psittaci infection, for which doxycycline has been suggested as a treatment option.” Each patient received one or two cycles of doxycycline (100 mg bid) for 3 weeks; 200 mg/daily for 3-6 wks. The outcome result was, “No serious adverse event was reported during doxycycline therapy". In conclusion, first-line doxycycline therapy was effective and safe.”


“Safety and efficacy of doxycycline in the treatment of rosacea”.
Where they treated patients with SDD 20 mg twice daily for 8 weeks, and after an average of 4 weeks, patients experienced an 80% to 100% clearing in inflammatory lesions and a 50% reduction in erythema. At the end of treatment, there were no reports of gastrointestinal side effects, vaginitis, or photosensitivity.
Another article I located in PubMed, where a clinical comparative study done with acne vulgaris patients receiving either single dose 50mg Doxycycline or two 50mg doses of minocycline over a 12 week period.


Comment made by Dr Guy Webster,(Professor of Dermatology, Jefferson Medical College, Philadelphia) in this article;
“Long-term Oral Antibiotics for Acne: Focus on Safety”
Excerpt; “We've all done studies showing that you can get patients to be weaned from oral antibiotics after several months if they have been started on topical retinoids simultaneously.”
When treating acne there is concern of resistant bacteria which makes ongoing uninterrupted treatment essential for success. Symptom relief is not considered clinically as a treatment success.


Medicines for the Prevention of Malaria While Traveling-CDC
Malaria treatment can include other drugs like plaquenil (Hydroxychloroquine) however just as a preventative step doxycycline is recommended prior to exposure, then continued for the duration of the trip/visit and then another 4 wks after potential exposure. Even a short visit to a malaria endemic area would make prophylactic treatment with antibiotics over 28 days.
When treating venereal disease where syphilis, another spirochete, is involved that treatment and testing is a 4 month process, including dark field staining as a diagnostic tool monthly to mark progress.

This review speaks loudly, long-term amoxicillin, ciprofloxacin, and doxycycline use appears safe; amoxicillin, ciprofloxacin, and doxycycline, does not appear to increase over time with prolonged exposure. (Meropol, Chan and Metlay) research confirmed in 2008 that the IDSA and CDC’s recommendation long term (60 days) use of amoxicillin, Cipro or Doxy as safe and supporting protocol if a community is exposed to Anthrax.
“The Infectious Diseases Society of America and US CDC recommend 60 days of ciprofloxacin, doxycycline or amoxicillin for anthrax prophylaxis. It is not possible to determine severe adverse drug event (ADE) risks from the few people thus far exposed to anthrax prophylaxis. This study’s objective was to estimate risks of severe ADEs associated with long-term ciprofloxacin, doxycycline and amoxicillin exposure using 3 large databases: one electronic medical record (General Practice Research Database) and two claims databases (UnitedHealthcare, HMO Research Network).”


So in conclusion; apparently taking doxy for more than 28 days is alright if you are treating VD with a side of syphilis, moderately severe acne, Rosacea. Just visiting a known Malaria infected area will get you 3 months of doxycycline, or in the treatment of Ocular adnexal lymphoma (OAL) and for treating anthrax exposure but not Lyme disease. So I ask you; is the medical community's concerns about antibiotic resistance or Lyme disease 'treatment' resistant?